
Soft Tissue Surgery
Maximising Success with Intestinal Suturing
Enterotomy and enterectomy are commonly performed procedures in practice due to the frequent occurrence of gastrointestinal foreign bodies. Although these are common procedures, good surgical technique is essential as the consequences of dehiscence are devastating with the development of septic peritonitis.
The mortality rate associated with septic peritonitis can be as high as 50%. Dehiscence rates following gastrointestinal surgery have been reported from 3-27%, however our experience would suggest that with good technique we should expect rates at the lower end of this range.
The following tips should help minimise complications with gastrointestinal surgery:
- Control contamination – pack the intestinal segment away from the abdomen with saline soaked swabs before starting surgery. Have an assistant digitally occlude the intestine either side of incision or place Doyen forceps to prevent contamination with bowel contents.
- Tissue handling – minimise handling and trauma to the tissue; using Debakey forceps is ideal.
- Suture pattern – simple interrupted appositional sutures. It is essential the submucosa is included in the suture bite as this is the strength-holding layer of the intestine. Take a good bite of intestine (2-3mm). Small bites are more likely to pull through.
- Suture size – 1.5 metric is the ideal size and is suitable for all small animals from cats to Great Danes.
- Suture material – a monofilament absorbable suture is best. Our preference is for PDS. Although commonly used in practice Polyglactin 910 (Vicryl) is not an ideal material for intestinal surgery as it is multifilament which has more drag and can result in bacteria wicking from the intestinal lumen.
- Suture spacing – place sutures approximately 3mm apart. A good guide is that you should not be able to place the tips of a closed pair of Debakey forceps between the sutures. Too many sutures placed too closely together can result in the necrosis of the intestinal edge and dehiscence due to damage to the blood supply.
- Leak testing – although advocated by some surgeons, we do not find this useful and do not routinely perform this technique.
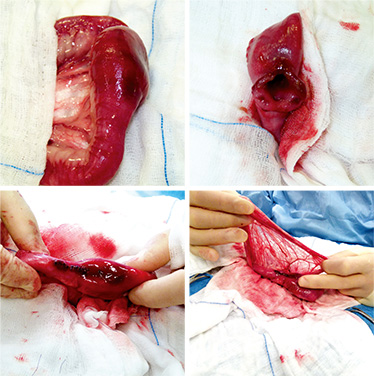
- Reinforcement – patching the suture line with omentum can significantly reduce the risk of dehiscence. This is due to its ability to produce a seal, provide neovascularistion and resolve infection. Place omentum over the suture line and hold in place with 4 simple interrupted partial thickness tacking sutures.
Case Advice or Arranging a Referral
If you are a veterinary professional and would like to discuss a case with one of our team, or require pre-referral advice about a patient, please call 01883 741449. Alternatively, to refer a case, please use the online referral form