
Primary brain tumours are common in dogs. Certain breeds such as Boston Terriers, Bulldogs, Boxers or Golden Retrievers are predisposed whereas others seem to be more resistant (Dobermans, Cocker Spaniels).
Clinical signs vary depending of the location and growth rate and include seizures, behavioural changes, decreased mentation, circling or vestibular signs. Signs of increased intracranial pressure appear when self-regulation mechanisms are overwhelmed. This can lead to a severe decrease in mentation, loss of pupillary light reflex, coma, opisthotonus, vestibular signs and death.
Types of Tumour
Meningioma
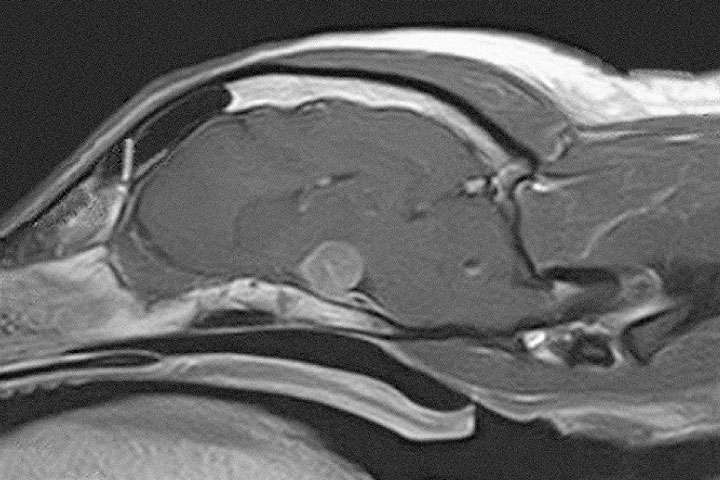
It is the most common primary brain tumour in dogs and cats. Meningiomas are extra-axial, well demarcated, large masses. As derived from the leptomeninges, they sit between the dura and the brain.
On MRI, they appear as well defined, homogeneous, broad base masses with strong and uniform contrast enhancement.
The majority of meningiomas are supratentorial (75%), but caudal fossa or skull base meningiomas are occasionally seen.
Surgical treatment is usually effective and peri-operative mortality relatively low (17%). In cats median survival times are 2 to 4 years after surgery with 80% of them being cured. Canine meningioma survival varies between studies, but some report times of more than 2000 days.
Medical treatment does not reduce the tumour size, but it may reduce tumour growth and alleviate clinical signs.

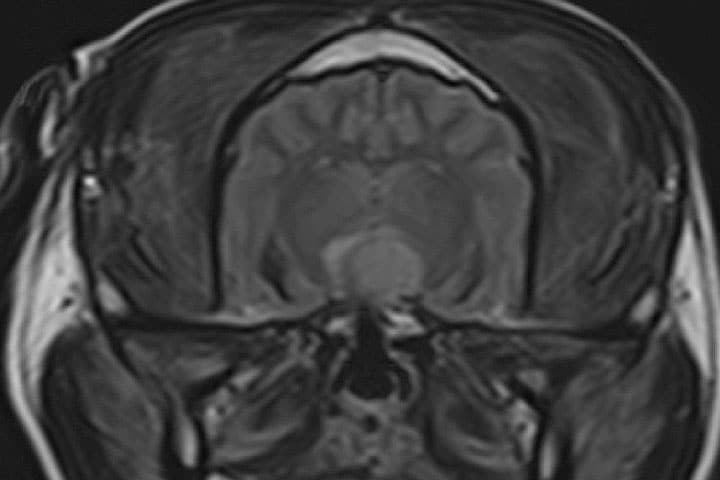
Pituitary masses
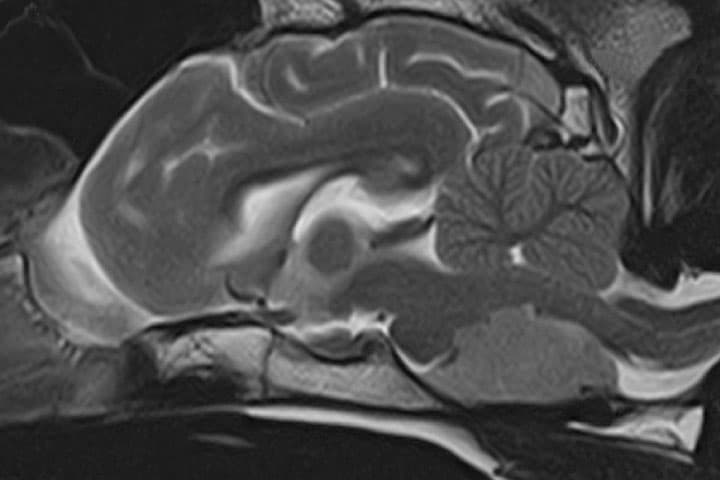
Pituitary adenomas or adenocarcinomas are the most common type of pituitary tumours. They can cause neurological signs by compressing the diencephalon. Clinical signs tend to be subtle and may only relate to hypothalamic dysfunction: low temperature, heart rate and decreased mentation. The oculomotor nerve (pupil size and eyeball movement) can be affected. On many occasions they cause hyperadrenocorticism.
On MRI or CT they appear as a single mass in the skull base-medial cranial fossa extending dorsally.

Surgery (hypophysectomy) reports median survival of >700 days, whereas new radiotherapy techniques can get longer survivals (2000 days) with less peri-operative mortality. Radiotherapy protocols however may not be accessible for all patients, and surgery is a very good alternative.
Palliative treatment tends not to be effective in relieving the neurological signs; deterioration tends to be slowly progressive. Surgery can potentially cure hyperadrenocorticism however hormone replacement therapy will be needed long term.
Germ cell tumours or craniopharyngiomas can also occur in this area, although they are rare in dogs.
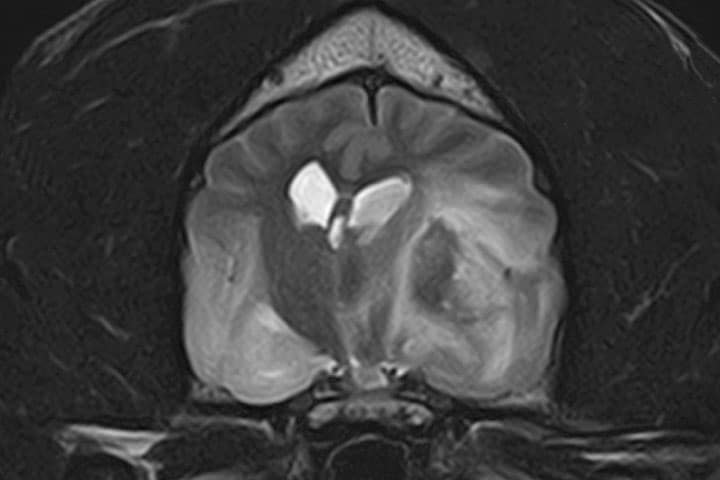
Choroid plexus tumours and Ependimomas
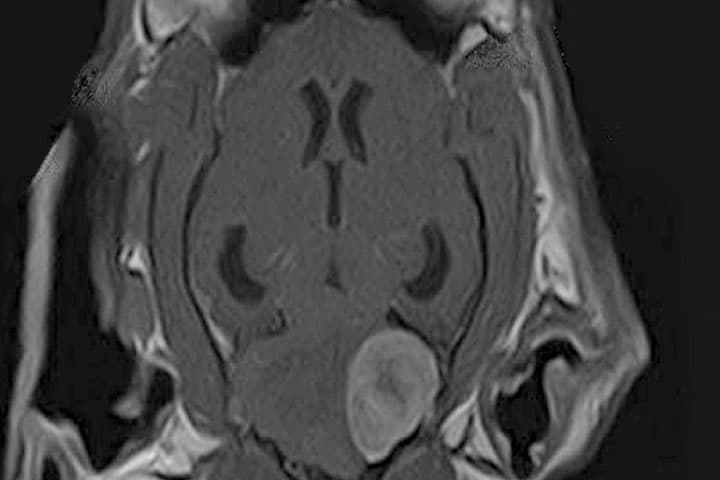
These intra-ventricular tumours cause hydrocephalus and diffuse bilateral symmetric forebrain signs.
They can be differentiated into Choroid Plexus Papilloma or Carcinoma with different growth rates and prognoses. Cerebrospinal fluid protein levels can help to differentiate between the two.
Currently, surgery is not attempted on these types of tumours, however intraventricular peritoneal shunting (VPS) can resolve signs of hydrocephalus temporarily. They usually carry a poor prognosis.
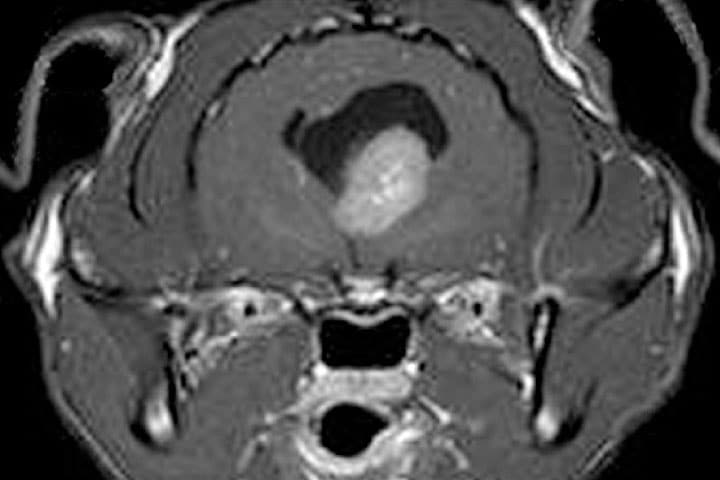
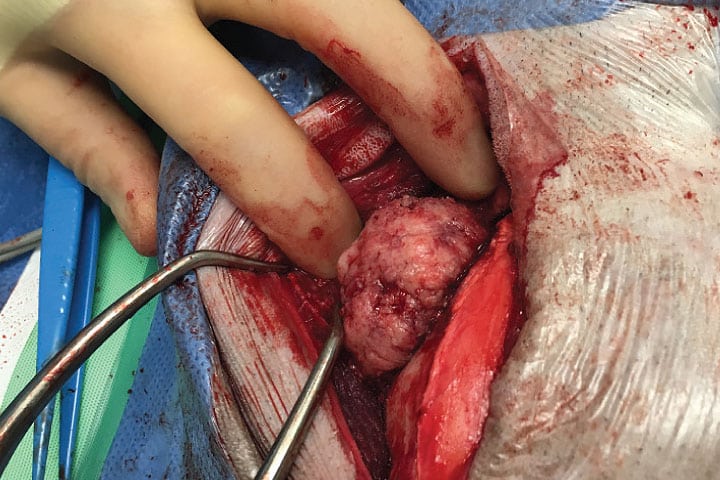
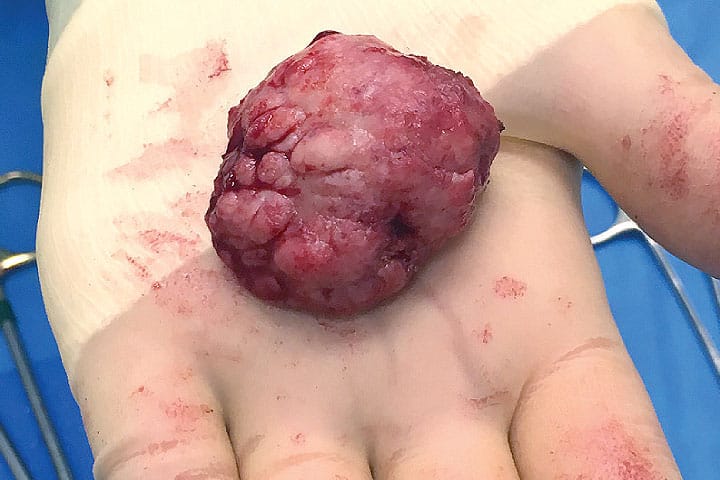
Multilobular Osteochondrosarcoma
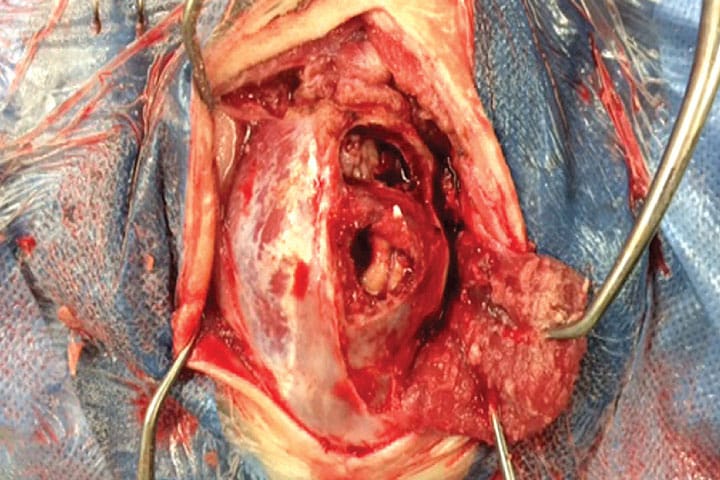
These are slow growing tumours that arise from the skull but can cause severe compression of the brain. Although not primary tumours, they may not be noticed until neurological signs appear. Surgery can be very successful in these cases.

Gliomas
Gliomas are the second most common primary brain tumour in dogs. They are more prevalent in brachycephalic breeds, but rare in cats.
On MRI they appear as intra-axial masses with mass effect and heterogeneous contrast uptake. Some can have accompanying signs of haemorrhage (T2* signal void).
Gliomas can be divided histopathologically in oligodendrogliomas and astrocytomas, with different grades of malignancy; from slow growing to highly aggressive glioblastoma multiforme or gliomatosis cerebri.
Surgery is usually not indicated due to difficult access and re-growth. Chemotherapy tends not to be very effective. Treatment consists of palliative medication (2-3 months survival) or radiotherapy (around 1 year).

Key messages
- Brain tumours do not always carry a death sentence
- Prognosis can be good even when neurological signs are marked
- Advances in radiotherapy and modern surgical techniques mean that dogs and cats can achieve long survival times while maintaining a very good quality of life
- Surgical resection is the treatment of choice in many types of tumours such as meningiomas, pituitary tumours and skull tumours.
Case Advice or Arranging a Referral
If you are a veterinary professional and would like to discuss a case with one of our team, or require pre-referral advice about a patient, please call 01883 741449. Alternatively, to refer a case, please use the online referral form
About The Discipline
Oncology

Need case advice or have any questions?
If you have any questions or would like advice on a case please call our dedicated vet line on 01883 741449 and ask to speak to one of our Oncology team.
Advice is freely available, even if the case cannot be referred.
Oncology Team
Our Oncology Team offer a caring, multi-disciplinary approach to all medical and surgical conditions.