
Clinical signs for Vestibular Syndrome can include a head tilt, wide base stance, vestibular ataxia, rolling or leaning to one side, pathological nystagmus (either spontaneous or positional), reduced oculocephalic reflex and strabismus.
Some of these signs are pathognomonic to vestibular disease, meaning that when present, they clearly indicate a problem in one of the anatomic components of the vestibular system (with the exception of occasional C1-C3 spinal cord lesions). These pathognomonic signs are pathological nystagmus and a head tilt.
Clinical signs of Vestibular Disease:
- Head tilt
- Vestibular ataxia
- Pathological nystagmus
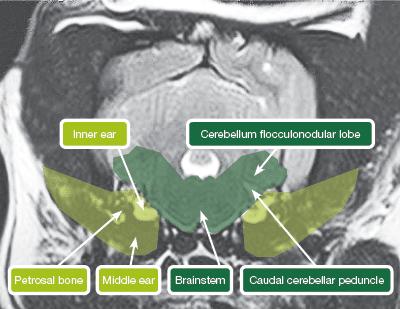
The anatomical areas that constitute the vestibular system are the inner ear, petrosal part of the temporal bone, the brainstem, the caudal cerebellar peduncle and the cerebellar flocculo-nodular lobe. For a clinical approach, we divide these anatomical areas into peripheral vestibular (including the inner ear and sometimes middle ear by extension and the petrosal bone) and central vestibular (brainstem and cerebellum). Lesions in these different areas can have distinctive clinical signs that can help in the localisation of the problem.

Tips for Peripheral Vestibular localisation:
- Normal mentation
- Normal postural reactions
- Can have Horner’s Syndrome (ipsilateral)
- Can have facial paralysis (ipsilateral)
- Fast rate of nystagmus (> 66bpm) in 95%
Common Peripheral Vestibular diseases
- Otitis interna/media
- Idiopathic – geriatric
- Ototoxic drugs
- Polyps
- Neoplasia
- Congenital – Doberman, Cocker Spaniel
- Hypothyroidism
Tips for Central Vestibular localisation
- Proprioceptive deficits in 95%
- Other cranial nerve deficits (60%)
- Decreased mentation (45%)
- Cerebellar signs
- Contralateral head tilt and proprioceptive deficits
- (paradoxical vestibular syndrome in cerebellar disease)
Common Central Vestibular diseases (VITAMIN D)
- Vascular – cerebrovascular accident (thalamus, cerebellum)
- Inflammatory/ infectious – (GME, FIP, Neospora)
- Toxic – metronidazole
- Anomalous – quadrigeminal cysts, hydrocephalus
- Metabolic- thiamine deficiency
- Neoplastic – meningioma, choroid plexus tumour at the cerebellopontine angle
Neurolocalisation in Vestibular Disease can be very helpful in determining what diagnostic tests to perform and when to refer for further imaging. It can also give an idea of differential diagnosis and prognosis. However, neurolocalisation is not a perfect system: one third of dogs that localise to peripheral vestibular can actually have a central lesion, so an MRI or CT scan should be offered for better assessment.
Case Advice or Arranging a Referral
If you are a veterinary professional and would like to discuss a case with one of our team, or require pre-referral advice about a patient, please call 01883 741449. Alternatively, to refer a case, please use the online referral form
About The Discipline
Neurology

Need case advice or have any questions?
If you have any questions or would like advice on a case please call our dedicated vet line on 01883 741449 and ask to speak to one of our Neurology team.
Advice is freely available, even if the case cannot be referred.
Neurology Team
Our Neurology Team offer a caring, multi-disciplinary approach to all medical and surgical conditions.