
There are different components that make up the precorneal tear film: lipid, aqueous and mucin. The lipid layer is the most superficial and is produced by the meibomian glands located within the eyelid margin. The aqueous component is produced by the orbital lacrimal gland and by the gland of the nictitating membrane. The mucous layer is secreted by the conjunctival goblets cells.
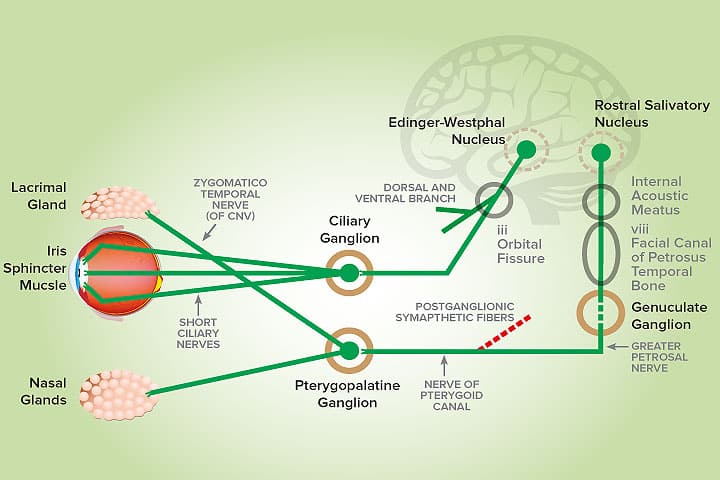
Aqueous production from the lacrimal gland is the result of a complex physiologic process. Both the basal and reflex tears are under the control of the autonomic nervous system. The afferent arm involves the trigeminal nerve (ophthalmic branch), while the efferent component involves the parasympathetic output into the lacrimal gland via the facial nerve.
The preganglionic neurons originate within the parasympathetic nucleus of the facial nerve, located within the rostral portion of the medulla oblongata. These fibres run as part of the facial nerve through the facial canal of the petrous temporal bone (middle ear), branching then into the major (greater) petrosal nerve that synapses with the pterygopalatine ganglion. The post-ganglionic axons innervate the lacrimal gland, the palatine and lateral nasal gland (the latter is very relevant when considering the clinical presentation of neurogenic keratoconjunctivitis sicca – KCS). The lacrimal gland is innervated by the zygomatic and lacrimal nerve (both branches of the trigeminal nerve).
Lesions affecting the efferent pathway will lead to a decrease in tear production and this condition is known as neurogenic KCS.
Clinical signs
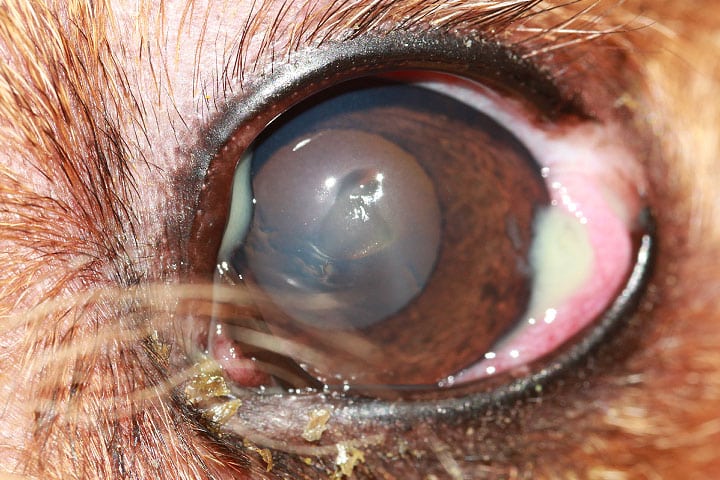
Patients typically present with an acute history of marked unilateral mucopurulent ocular discharge (Figure 1). Schirmer tear test readings are significantly different between both eyes. The affected eye will normally be lower than 5mm/min and the contralateral eye will be normal. Further examination often identifies a dry nostril (xeromycteria) ipsilateral to the dry eye (Figure 2).

Most patients do not have additional clinical signs. However, other neurological deficits can be detected concurrently depending on the localisation of the lesion, namely: Horner’s syndrome (the sympathetic nerves pass in close proximity to the inner/medial ear) and facial paralysis if the preganglionic nerve (major petrosal nerve) is affected (eg: otitis media and/or interna, petrositis). Erosive lesions to the floor of the medial fossa of the skull can lead to trigeminal nerve deficits such as facial anaesthesia and xeromycteria (dry nasal mucous membranes). Injuries to the pterygopalatine fossa could include periorbital myositis, cellulitis and dental abscessation. Post-ganglionic lesions are commonly identified in cases of orbital trauma.
Other causes
Other possible causes of dry eye should be ruled out such as: immune-mediated disease (typically bilateral and often of a more gradual onset), congenital (eg: Yorkshire Terrier and English Cocker Spaniel), iatrogenic (eg: excision of nictitating membrane gland), traumatic, infectious (eg: canine distemper virus), radiation therapy, drug-induced (eg: sulphonamides and atropine) and systemic diseases (eg: diabetes mellitus and hypothyroidism). Ideally advanced imaging (eg: CT scan or MRI) should be performed in order to identify possible lesions. However, given that the majority of canine neurogenic KCS cases are idiopathic and in the absence of other neurological deficits these tests do not always need to be performed.
Pilocarpine is normally given 2 to 3 times daily, 1 drop per 10Kg of bodyweight. The dose is gradually increased by one drop increments (eg: every 2 to 3 days) until there are signs of gastrointestinal toxicity (hypersalivation, inappetence, vomiting and diarrhoea).
Once these signs are detected, treatment is temporarily discontinued for 24 hours and the dose is lowered to the previously highest tolerated dosage.
There are anecdotal reports where topical 0.125 – 0.25% pilocarpine solution diluted in artificial tears is used but the results are not consistent, and the drug can be irritant when applied directly in the eye.
Some dogs, however, may respond to prolonged systemic broad-spectrum antibiotics and non-steroidal anti-inflammatories when an underlying infectious/inflammatory process is responsible.
Topical cyclosporine has been used concurrently in some patients and although the success of therapy is more relevant in patients with dry eye due to immune-mediate disease, its mucinogenic effect may be beneficial.
The prognosis for dogs suffering for neurogenic KCS is dependent upon the response to treatment. The mainstay of medical therapy includes topical tear replacements and the use of oral 1-2% pilocarpine, a direct-acting parasympathomimetic drug. Response to therapy is secondary to parasympathetic denervation, in which peripheral cholinergic receptors have undergone upregulation and are more sensitive to the effects of cholinergic stimulation than other cholinergically innervated tissues, also known as denervation hypersensitivity.
Reported success rates of treatment are generally poor, but in one case report approximately 50% of the patients (5 of 11 dogs) recovered within 125 days of diagnosis. According to this study neurogenic KCS was predominantly an idiopathic disease.
If response to medical therapy is not satisfactory, surgery is available in the form of parotid duct transposition. However, this procedure needs to be carefully and thoroughly discussed with the owners due to possible complications encountered with this surgery. Nonetheless, recent studies have reported a high overall success rate and high owner’s satisfaction following the procedure.
- Neurogenic KCS is a relatively uncommon condition.
- It is vital to recognise the characteristic clinical signs in order to choose the appropriate treatment and give an accurate prognosis.
- Patients may present with an acute onset, severe unilateral dry eye and frequent ipsilateral dry nasal planum.
- A dry nasal planum (xeromycteria) is a result of the deficient parasympathetic innervation of the lateral nasal gland.
- Parotid duct transposition surgery can be considered in patients refractory to medical therapy.
References:
Featherstone H, Holt E. (2011) Small Animal Ophthalmology: What’s Your Diagnosis? Wiley-Blackwell.
Rhodes M (2014). Canine keratoconjunctivitis sicca: an overview. Companion animal 19 (7): 336-40
Matheis Fl, Walser-Reinhardt L, Speiss Bm (2012). Canine neurogenic keratoconjunctivitis sicca: 11 cases (2006-2010). Veterinary Ophthalmology 15 (4): 288-90
Webb AA, Cullen CL. Neuro-ophthalmology. In: Gelatt KN (ed.) Veterinary Ophthalmology. 5th ed. Ames, Iowa: John Wiley & Sons, Inc.
Garosi L, Lowrie M. Neuro-ophthalmology. In: Gould & Mclellan (ed.) BSAVA Manual of Canine and Feline Ophthalmology. 3rd ed. Quedgeley, Gloucester: BSAVA.
Miller P. Lacrimal system. In: Maggs, Miller & Ofri (ed.) Slatter’s Fundamentals of Veterinary Ophthalmology
Rhodes M, Heinrich C, Featherstone H et al (2012). Parotid duct transposition in dogs: a retrospective review of 92 eyes from 1999 to 2009. Veterinary Ophthalmology 15 (4): 213-22
Case Advice or Arranging a Referral
If you are a veterinary professional and would like to discuss a case with one of our team, or require pre-referral advice about a patient, please call 01883 741449. Alternatively, to refer a case, please use the online referral form
About The Discipline
Ophthalmology

Need case advice or have any questions?
If you have any questions or would like advice on a case please call our dedicated vet line on 01883 741449 and ask to speak to one of our Ophthalmology team.
Advice is freely available, even if the case cannot be referred.
Ophthalmology Team
Our Ophthalmology Team offer a caring, multi-disciplinary approach to all medical and surgical conditions.