
Liver disease can be associated with specific clinical signs such as jaundice, non-specific clinical signs such as hyporexia, or can be asymptomatic and discovered incidentally when performing biochemistry tests for other reasons.
It is important to be aware that liver disease may be primary (inflammatory hepatopathies, copper accumulation etc), or secondary to other pathologies within the portal system (eg reactive hepatopathies commonly seen secondary to gastrointestinal pathology).
When investigating liver disease, a good understanding of the pros and cons of each test is important. The following considerations might be useful additions to your knowledge:
Liver enzymes
- Liver enzyme elevations of course often infer hepatic damage, but cannot be used to indicate chronicity, liver function, or potential reversibility.
- The half-lives of liver enzymes are very different in cats and dogs (around 10x shorter in cats)- so any elevation in a cat is relevant.
- Different liver enzymes have different sensitivities and specificities to consider: for example ALT is elevated in 80% of dogs with liver disease, but in only 50% of cats however very few cats with normal livers will show an elevated ALT, so it is a very specific marker in cats, whereas in dogs, the specificity is only 50%.
- GGT is the most sensitive indicator of feline hepatobiliary disease
Bile acid stimulation test
- Bile acid stimulation tests in jaundiced animals in which haemolysis has been excluded won’t be useful- both hepatic and post-hepatic (biliary) causes of jaundice will be associated with marked elevations in bile acids.
- Massive elevations of bile acids (>80-100 mmol/l) are strongly supportive of portosystemic shunting (either congenital or acquired), but mild elevations can be seen in both primary and secondary liver disease (for example bile acids pre or post-prandially of 30-45 mmol/l are common in dogs with hyperadrenocorticism, likely reflective of the vacuolar hepatopathy that is commonly present).

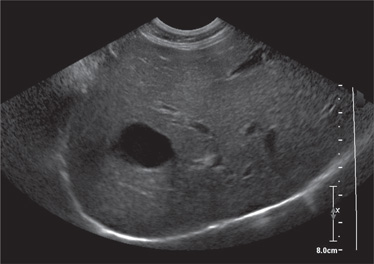
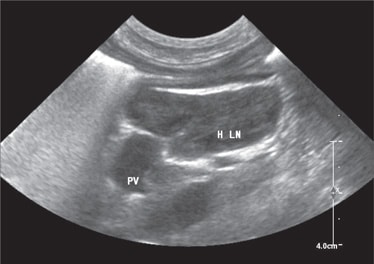
Abdominal ultrasound
- Ultrasound is a relatively insensitive test for confirmation, or identification of liver disease generally: for example only 48% of dogs with inflammatory hepatopathy, 69% of dogs with fibrosis and 68% of dogs with lymphoma will show abnormal liver on ultrasound. It is really important thus to realise that a liver of normal size and echogenicity does not exclude significant hepatic disease.
- There are many variations in the ultrasound appearance of one specific disease too: for example lymphoma may show as a mass lesion, heterogeneity, or a diffusely hyperechoic, hypoechoic or isoechoic liver.
- There are of course some findings both in the liver (target lesions) and in the wider abdomen (significant lymphadenopathy, abdominal effusion, splenic masses) which may be more helpful to further investigate to determine the cause of a liver abnormality.

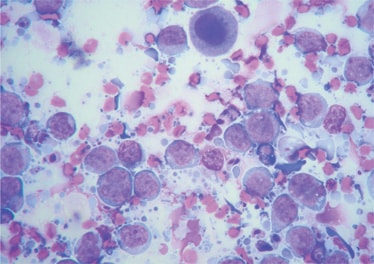
Cytology of hepatic aspirates
- The agreement between cytology and histopathology for many types of liver disease is very disappointment, and when assessing liver disease as a whole, the agreement is only 30-40%.
- Cytology is good for identifying some diseases, such as lymphoma, and vacuolar change would be expected to be identified cytologically too (although this is a non-specific finding, and the most common misdiagnosis on cytology).
- Architectural changes (fibrosis, portal vein hypoplasia) cannot be appreciated cytologically, and inflammation is rarely accurately detected.
Histopathology of hepatic biopsies
- In most instances, liver biopsies are the best way to determine the nature of liver changes. These can be obtained with ultrasoundguided Trucut, laparoscopy or surgery.
- Coagulation times, and platelet count assessment are suggested prior to any of these procedures to minimise the potential for procedure-related haemorrhage.
While all of these diagnostics can be useful in determining the nature of liver pathology, it is important to be aware of the limitations of each test, to prevent inappropriate exclusion of differential diagnoses, and plan your next step appropriately.
Case Advice or Arranging a Referral
If you are a veterinary professional and would like to discuss a case with one of our team, or require pre-referral advice about a patient, please call 01883 741449. Alternatively, to refer a case, please use the online referral form
About The Discipline
Internal Medicine

Need case advice or have any questions?
If you have any questions or would like advice on a case please call our dedicated vet line on 01883 741449 and ask to speak to one of our Internal Medicine team.
Advice is freely available, even if the case cannot be referred.
Internal Medicine Team
Our Internal Medicine Team offer a caring, multi-disciplinary approach to all medical and surgical conditions.